



Over the study period 51 responses were received, 49 of which were fully completed, with an average completion time of 46 min.
Importance
Overall, bedside audit items scored as most important to be included in future audits were: diabetes type (1.0), documented evidence of patient being seen by the inpatient diabetes team (1.0), reason for admission (0.99), and treatment regimen (0.99). Bedside audit clinical items rated as relatively least important included: smoking history in pack-years (0.43), excess days on intravenous insulin infusion (0.48), and time of day of hypoglycaemia occurrence (0.50).
Audit items in hospital healthcare delivery that scored as most important included: prevalence of diabetes in hospitalised patients (0.94) and presence of a multidisciplinary foot care team (MDFT) (0.93). The audit items rated as relatively least important included: presence of a triage system for risk stratification of diabetes severity (0.77), difficulties in accessing specialists for inpatient diabetes care (0.77), and types of population seen by MDFT (0.79).
Items in patient healthcare experience survey scored generally low in importance compared to other sections. Audit items that scored as the most important included: patient’s level of satisfaction on overall care of their diabetes (0.80) and patient’s perception of the appropriateness of the knowledge level of their ward staff member on diabetes (0.75). The items rated as the least important included ward staff ability to respond to patients’ questions about diabetes (0.60) and the inclusion of a patient experience survey (0.64).
Feasibility
Bedside clinical audit items rated as most feasible were patient age (0.97) and gender (0.96) while low overall feasibility scores were given to items regarding excess days on intravenous insulin infusion (0.39), smoking history in pack-years (0.40), duration of diabetes (0.44), and body mass index (BMI) (0.47). Healthcare delivery audit items considered to be highly feasible were the presence of a seven day per week diabetes educator service (0.86), the presence of a MDFT (0.86), and the presence of a seven day per week diabetes management consult service (0.85). Items from the hospital characteristics survey with lower feasibility scores included: difficulties in accessing specialists (0.66), presence of a triage system (0.71), and presence of an electronic system integrated with web-linked blood glucose meters enabling an alert system to ward staff (0.72). Feasibility was not surveyed for the majority of items in the patient experience survey. A feasibility score was obtained for whether the patient was involved in diabetes treatment planning (0.44) and the inclusion of a patient experience survey (0.59), which were generally lower than those in other sections.
Feasibility vs. importance
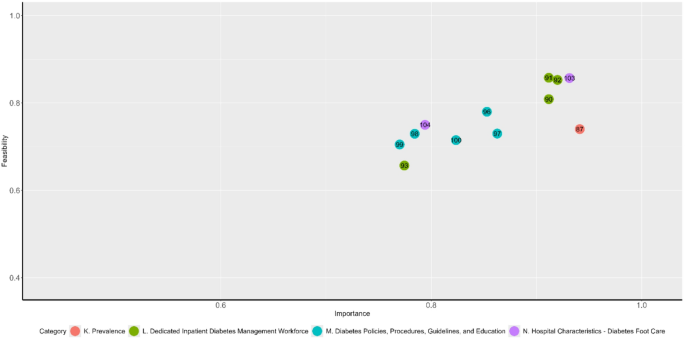
When feasibility is graphically compared with importance it is evident that for most items as mean relative importance increases so does mean feasibility (Figs. 1 and 2). Of the various sections of the bedside audit survey, items from the “background information” and “involvement of the specialist diabetes team” sections had generally high importance and feasibility scores while items from the “self-management”, “prescribing and drug management errors”, and “intravenous insulin infusions” had generally lower ratings. Ratings for items in the “general foot care” and “pre-operative care planning” sections were clustered around the median for all items, which are 0.70 and 0.83 for feasibility and importance respectively. The “patient details” and “glycaemic control and patient harm” sections included items that attracted both high and low importance and feasibility ratings.

Hospital characteristics audit fields
There were some items with notably discordant mean relative importance and feasibility. Item 60 regarding the presence of documentation of a diabetic foot risk examination in the first 24 h of admission (Item 60) was considered relatively feasible but unimportant. Patient’s BMI (Item 20) and duration of diabetes (Item 18) were rated as being relatively unfeasible compared with other items given a similar mean relative importance score.
Similar to the bedside audit items, mean relative importance of hospital characteristics audit items increased with mean feasibility (Fig. 2). Items from the “prevalence” and “diabetes foot care” sections attracted high ratings. While prevalence of diabetes in hospitalised patients (Item 87) was rated as being highly important, its feasibility was significantly lower than items given a similar relative importance. The median values for hospital characteristics audit items were 0.75 and 0.86 respectively.
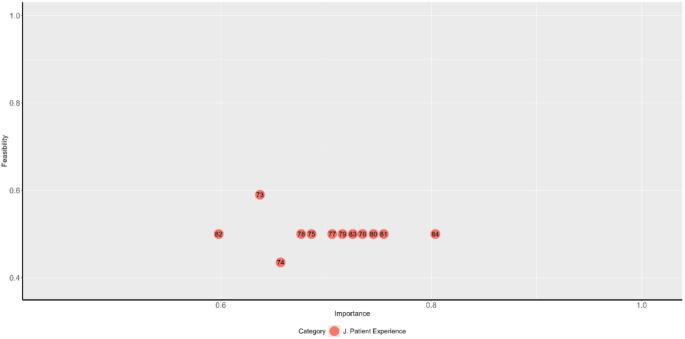
Since feasibility was not surveyed for most patient experience survey items, for the purpose of graphical representation these items are depicted with a feasibility of 0.50 (Fig. 3).
Patient healthcare experience audit fields
Free text responses
The free text “feedback” items provided further insights into how the planned audit could be improved and described why specific fields had scored in particular ways.
For the “background information” section, the free text responses suggested considering the pregnancy-related diabetes patient population as one of the options in audits. Several comments remarked on how feasibility can differ by admitting specialty, even within an institution, but also depend on whether the institution uses an electronic medical record (EMR) system.
For the “patient demographics” section, there was a comment suggesting clarification on whether the audit would ask for patients’ biological sex or gender identity. Several respondents remarked on the time-consuming and subjective nature of collecting diabetes complications information. Some comments enquired about the relevance of the smoking history and pack years in improving inpatient diabetes care. Many commented on the low feasibility of attaining the patient’s BMI from records, as height and weight are infrequently recorded. Some respondents questioned the value of collecting self-management data, currently one of the audit sections, in assessing the quality of inpatient diabetes management.
Regarding institutional glycaemic management, some commented on the time-consuming nature of gathering such data. There were discrepancies in respondents’ perceptions of which audit fields best reflect glycaemic management in an inpatient setting, especially the definition of “good diabetes days”.
In the “prescribing and drug management errors” section, several respondents commented that many of the audit fields on intravenous insulin infusions are highly subjective and time-consuming as they require clinical judgement.
The “patient experience” section was considered low importance and feasibility, and the feedback reflected the many barriers to patients completing surveys, including health literacy and proficiency in the English language.
In summary, the free text comments generally expressed concerns about the time-consuming nature of inpatient diabetes audits for clinicians and the potential requirement for purpose-specific auditors to ease the auditing burden on clinicians, particularly for those working in institutions that do not use an EMR.
link