
Impact of sex and menopausal hormonal therapy on cardiovascular diseases in people with diabetes or prediabetes

Data source
We utilized the National Health Insurance Service database from January 1, 2009, to December 31, 2019. Data were assessed for research purposes from August 31, 2023, to September 15, 2023. The National Health Insurance Service is a population-based cohort that conducts health screenings based on national health insurance data in Korea.
Informed consent
was not obtained as the study data had already been collected. The Institutional Review Board (IRB) of Ewha Womans University Mokdong Hospital approved our study. Due to the retrospective nature of the study, IRB of Ewha Womans University Mokdong Hospital waived the need of obtaining informed consent. Patient records were anonymized before release. All methods were performed in accordance with relevant guidelines and regulations.
Study population
The study included adults aged 40 years or older who underwent a health checkup between January 1, 2009, and December 31, 2010 (n = 2,688,352). Excluding those with missing data, the study population was 2,640,389. After excluding individuals with an estimated glomerular filtration rate (eGFR) < 15 mL/min/1.73 m2 (n = 47,452), with a history of chronic kidney disease indicated by ICD-10 codes N18 or N19 (n = 15,913), undergoing hemodialysis (n = 3,115), or with a history of heart failure (n = 59,177), the study population reached 2,523,352. Among them, 2,203,775 people were with prediabetes or diabetes. Finally, we analyzed 1,313,591 people with prediabetes and 890,184 people with diabetes. Additionally, we examined 1,180,576 people with prediabetes and 673,688 people with diabetes without a history of acute myocardial infarction or stroke. Participants were observed until the earliest occurrence of a CVD event, death, or the last follow-up on December 31, 2019. A flowchart detailing the participant selection process is shown in Fig. 1.
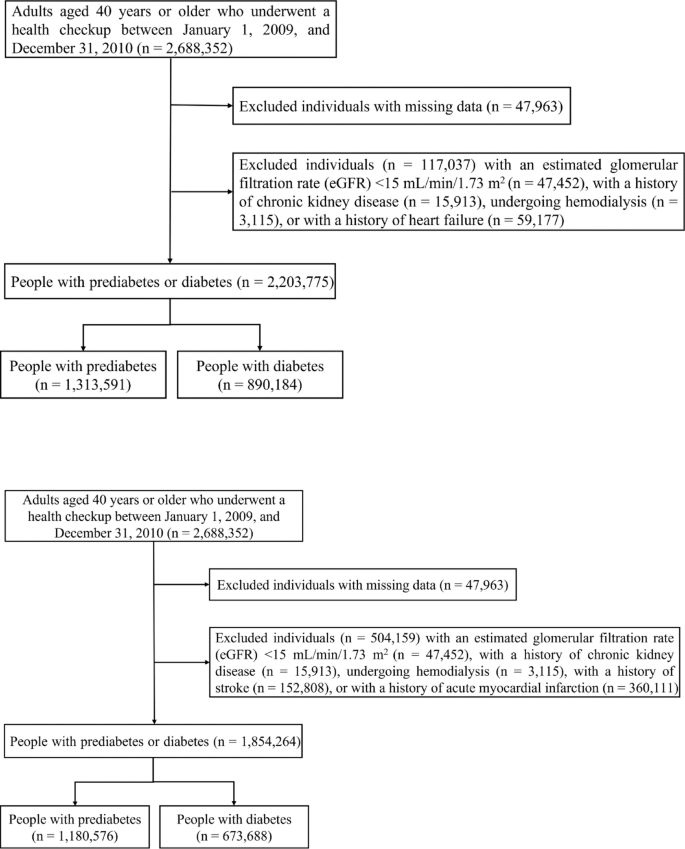
Flowchart detailing the participant selection process.
Diabetes was defined by the E10–14 codes of the 10th edition of the International Classification of Diseases (ICD-10) a prescription for oral glucose-lowering medications or insulin for more than 30 days or fasting glucose of 126 mg/dL or higher. Prediabetes was defined as fasting glucose between 100 and 125 mg/dL without meeting the diagnostic criteria for diabetes. Menopausal status was determined by having an ICD-10 code (N95), being over 60 years old, or using a self-report questionnaire.
Outcome variables and covariates
The primary outcome was the time to CVD occurrence, identified using ICD-10 codes: I21 for acute myocardial infarction, I60–I62 for hemorrhagic stroke, I63 for ischemic stroke, I60–I63 for stroke, and I50 for heart failure.
Smoking status was categorized as a current smoker or non/ex-smoker. Alcohol consumption was classified as heavy drinking (> 2 drinks/day for men and > 1 drink/day for women) or non-heavy drinking (≤ 2 drinks/day for men and ≤ 1 drink/day for women). Physical activity was grouped into none, 1 time/week, and ≥ 2 times/week.
Drug prescriptions at the index date were defined as those prescribed for > 30 days. Sociodemographic data (age, sex, smoking status, alcohol consumption, physical activity, and menopausal status for women), physical examination data (body mass index and blood pressure), laboratory test data (fasting glucose, cholesterol, and triglycerides), and treatment data (use of hypoglycemic agents, antihypertensives, and lipid-lowering therapies) were collected at the index date. The index date was the time of health screening after January 1, 2009, and the follow-up period from the index date to the occurrence of CVD, death, or the end of the study on December 31, 2019.
Statistical analysis
Baseline characteristics were presented as mean ± standard deviations for continuous variables and as frequency and proportion for categorical variables. We used Cox proportional hazards models to evaluate the risk of CVD events, adjusting for age, smoking status, alcohol consumption, physical activity, drug prescriptions for antihypertensives and lipid-lowering therapies, body mass index, and fasting glucose. Adjusted hazard ratios (HRs) and 95% confidence intervals were then calculated. P values < 0.05 were considered statistically significant. All statistical analyses were performed using SAS (version 9.4, SAS Institute, Cary, NC).
link




